Adult social care provider information provisions: guidance for providers on data collection
Updated 15 April 2025
Applies to England

© Crown copyright 2025
This publication is licensed under the terms of the Open Government Licence v3.0 ŇÁČËÖ±˛Ą. To view this licence, visit or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at /government/publications/adult-social-care-provider-information-provisions-data-collection/adult-social-care-provider-information-provisions-guidance-for-providers-on-data-collection
Background
High-quality reliable data, transparently and safely shared with those who can make good use of it, supports the functioning of the adult social care (ASC) sector. It supports high-quality commissioning, systems assurance and management of risks at a local, regional and national level.
The COVID-19 pandemic exposed challenges in bringing together data needed to effectively manage outbreaks and ensure that emerging risks and issues could be identified at all levels and appropriate action taken. This has highlighted the importance of having robust data flows in the ASC sector to provide assurance that local and national government have the data and local intelligence to provide oversight and national support where it is needed in the longer term. In turn, this will help ensure that ASCÂ data is used to benefit the sector and support people to make informed choices about their care.
Emergency data measures taken in response to COVID-19 gave us near real-time data to manage the pandemic and have shown us the benefits of using data to respond to emerging risks and issues.
Data from social care providers was critical to the government’s COVID-19 response and is continuing to help us:
- gain crucial insight into capacity and risk in the care system
- judge when and how to target support to providers
- facilitate the delivery of care and support to individuals across the care system
We are working closely with sector partners and key national organisations who use health and ASC data to ensure the most efficient methods of data collection and improvement in the interoperability of systems. We have committed to ensuring that the data architecture underpinning the health and care system can easily work together to make more effective and efficient use of data.
The received Royal Assent in April 2022. It includes:
1. A power for the Secretary of State for Health and Social Care to require adult social care providers to provide information relating to themselves, to their activities in connection with the provision of ASC in England or to persons to whom they have provided such care (section 99).
This power commenced on 31 July 2022 and applies to all ASC providers regulated by the Care Quality Commission (CQC). These are providers required to be registered under the Health and Social Care Act 2008 in respect of the carrying on of a regulated activity involving, or connected with, the provision of ASC in, or in relation to, England.
2. A power to make regulations enabling the Secretary of State for Health and Social Care to impose a financial penalty on private providers that do not comply with an information request or provide false or misleading information without reasonable excuse (section 100).
The were made on 10 November 2022 and came into force on 1 December 2022. Enforcement regulations apply to all private ASC providers regulated by CQC.
Data collection
Information required from 31 July 2022
From 31 July 2022, we mandated a core subset of the data which providers have already been submitting through the Capacity Tracker (CT). This is gathered on a monthly basis. Providers are required to update the CT with the required data within a designated 7-day reporting window. This window will open at the start of the 8th day of each month and run until the end of the 14th day of each month, or the next working day where the 14th day falls on a weekend or public holiday. This is shown in the graphics below.
Figure 1: data collection reporting windows
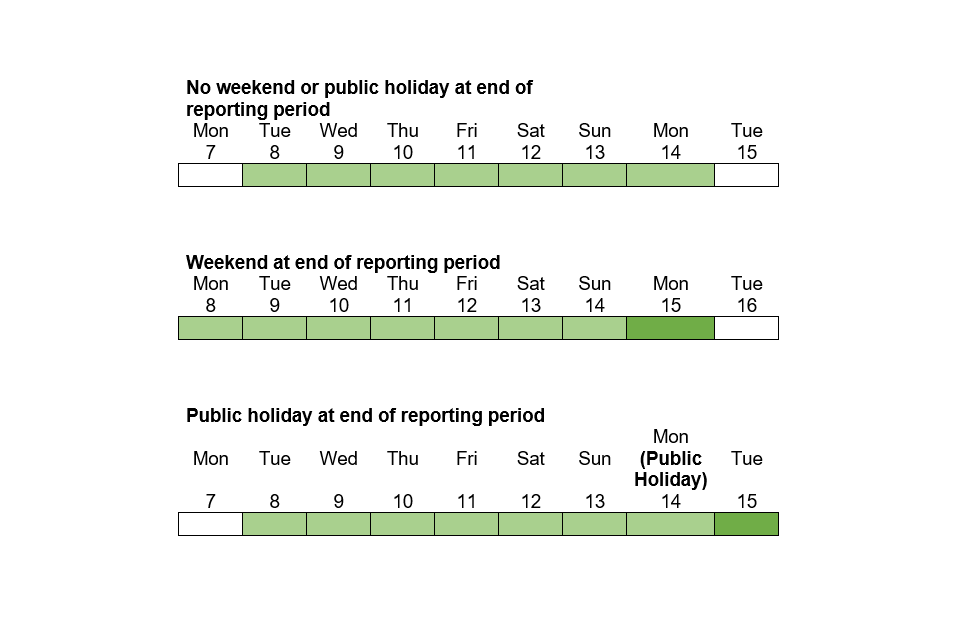
Figure 1 shows 3 graphics of the reporting windows:
- graphic 1 shows the reporting window if the 14th day falls on a weekday. The window is highlighted as being between the 8th and the 14th inclusive (both dates included)
- graphic 2 shows the reporting window if the 14th day falls on a Sunday. The window is highlighted as being between the 8th and the 15th inclusive (both dates included), which is the next working day from the Sunday
- graphic 3 shows the reporting window if the 14th day falls on a Monday and it is a public holiday. The window is highlighted as being between the 8th and the 15th inclusive (both dates included), which is the next working day from the Monday
Full dates to December 2030 are in Annex A.
Updates for this data will need to be made via the CT using the same method as at the time of this guidance’s publication - by providers either updating each mandated field individually or by the bulk update functionality. The data must be reviewed within the reporting window of each month, and, even if there are no changes to be made, the page is saved so that it is marked in the system as having been updated.
In November 2022, the Capacity Tracker Data Advisory Group (CTDAG) was replaced by the Provider Data Advisory Group (PDAG). As we did with CTDAG, DHSC will regularly engage with and consult the PDAG on:
- ways to make it clearer how data is being used centrally
- improvements to the wording and content of specific data items based on feedback received from ASC providers and data users
This is intended to ensure that any changes improve data quality and relevance, while also managing data burdens on providers.
PDAG membership includes representatives from:
- Association of Directors of Adult Social Services
- Care Software Providers Association
- CQC
- DHSC
- Department for Levelling Up, Housing and Communities
- Digital Social Care
- Local Government Association
- National Institute for Health and Care Excellence
- NHS England
- Professional Records Standards Body
- Skills for Care
The following provider groups are also PDAG members:
- Associated Retirement Community Operators
- Care Association Alliance
- Care England
- Care Provider Alliance
- Homecare Association
- Learning Disability England
- National Care Association
- National Care Forum
- Registered Nursing Home Association
- Think Local Act Personal
Other data items in CT are often key for local operational support and providers will be asked to provide more regular updates to these items - for example, daily bed vacancy updates and workforce data. Such data requests are separate to the mandated list but are essential to continue to support you as providers, and health and social care partners, such as discharge teams, to keep people and staff as safe and healthy as possible. The daily vacancy data is useful when more frequent because it supports people to be in the right place for their specific needs.
Data items that form part of the mandatory collection are clearly marked in the CT system during the reporting window period.
The latest list of data items can be found in the formal notice of a mandate for all adult social care providers.
Purpose of collecting this information
Availability of good quality and timely data from ASC providers is essential to:
- supporting efficient commissioning and systems assurance
- managing national, regional and local risks
- assisting with evolving situations, like COVID-19
- ultimately, helping to facilitate the care of individuals
Data mandation will build on the stronger data sharing practices we have built during the COVID-19 pandemic where providers have shared data and information using the CT tool. This has highlighted the importance of having robust data flows in the ASC sector to ensure that the right level of capacity and support is available for service continuity. It will support a consistent and transparent approach to the processing of data across privately and publicly funded care to support improved safety and quality of provision.
Data is needed to:
- continue to support COVID-19 recovery
- monitor vaccination levels
- understand capacity and risk in the care system more generally
- understand the impact of winter pressures
- determine when and how to target support to providers
- ultimately, help facilitate the care of individuals across the care system in the long term
For example, during the pandemic, provider data-sharing facilitated:
- flagging a need for a visit from a COVID-19 vaccination team - vaccination teams also used data to arrange visits directly
- highlighting issues with accessing flu vaccinations
- flagging PPE shortages
- receipt of targeted support from regional teams, using data from the workforce RAG status
- visualising and benchmarking your own provider data against local authority, regional and national data to understand how it compares
Emergency data measures taken in response to COVID-19 gave us near real-time data to manage the pandemic and showed the benefits of using data to respond to emerging risks and issues - for example, in outbreak management and prioritising PPE supplies for providers in highest need.
Currently, providers are able to view their data in the CT and use this for benchmarking purposes, comparing against the local authority, regional and national aggregate. This provider view will be reviewed and improved to better meet provider needs and support them to realise the full value of their data, noting such needs will differ depending on provider characteristics. We will be seeking feedback from providers on how to improve this view using the PDAG member organisations. Furthermore, we are keen to explore what wider data sources we can add to this view, to offer a richer source of data to providers that they would not be able to access without it.
Data also helps us to identify issues at an early stage and provide an evidence base for central government funding discussions. For example, CT data on staff absence in January 2021 showed the need for support with recruitment and that additional staff hours were needed, one of the drivers of the ÂŁ120 million Workforce Capacity Fund being established.
With more and better data, we can plan the future care of our population and will have the potential to generate significant health and care benefits such as:
- increased independence
- improved quality of care
- higher satisfaction for people drawing on health and care support
- more efficient use of funding
Improved data on the ASC workforce can also benefit recruitment, retention and equality policies.
We have carried out an impact assessment in relation to the financial implications of mandatory completion of the CT.
Engaging on future changes
The burden on ASC providers in providing data is a key consideration in all changes. Our aim is to reduce the burden overall where possible, while also improving the information data gives. If the data needs of DHSC or other ASC partners evolve or issues with data arise, wherever possible, we will give at least 3 months’ notice of any change to the mandated data listed above or to the frequency of collection before making it a legal requirement. If DHSC receive feedback on the usefulness or burden of the above listed data items, we will work with the sector to review and improve these as needed.
We intend to engage on changes with providers and representatives through the PDAG. The PDAG includes provider and local authority representatives.
If a change to a data item or a new data item is required by DHSC, DHSC will first consider key criteria such as whether it can be obtained elsewhere, what any output will be used for and the benefit of collecting it for providers, settings and other sector partners. If the need is clear, an example of how the data item will appear in the CT will be shared with PDAG for feedback and further iteration as part of co-building.
Depending on the scale of the change, any engagement might be solely via email feedback, representations at a PDAG meeting itself, or could involve workshop sessions. This iterative process seeks to refine the new or changed data item to a point where it is ready for development and adding to the collection. Once the process is complete, we will notify providers of the upcoming change, giving at least 3 months’ notice, where possible.
Support and guidance
Filling in the Capacity Tracker
The CT is managed by the North of England Care System Support (NECS) unit. NECS provides a dedicated support centre - Monday to Friday, 8am to 5pm - to support care providers and wider stakeholder users of the CT. If providers need support completing or updating the system, accessing or using the reports and analytics, they can reach out either by phone 0191 691 3729 or by emailing necsu.capacitytracker@nhs.net.
In addition, – all communications, reporting window open and closure dates, user or help guides and video tutorials along with contact details for local System Champions can be found there. You will need to sign in using your CT account details to access the resource centre.
NECS also utilises regional leads that are split across the 7 NHS England regions. They run regular provider engagement sessions and have set up regional forums to help support continuous improvement of the system and support our user centred design approach.
For guidance relating to how to answer specific questions, you can email capacitytracker-guidance@dhsc.gov.uk.
Providers will be contacted when they have not updated their CT data and will be offered support or advice on completing the return. Contact will be made through NECS or by other routes depending on the issue. Contact will normally be established by a combination of emails, telephone calls and NECS regional leads and local system champions.
For administrative amendments, account support and more, you can contact NECS directly already at: necsu.capacitytracker@nhs.net.
Data use and privacy
These provisions will not enable data to be sold to private organisations. Our intention is that data collected will be shared appropriately with organisations who need the data across the ASC sector (for example, local authorities, CQC, integrated care systems) to guide delivery, policy development and research in the area for purposes connected with the health or ASC system in England. We will continue to encourage all such partners to look to data in CT in the first instance rather than instigating separate data collections covering similar data.
The information will be subject to the UK General Data Protection Regulation (GDPR) and statutory restrictions on disclosure. This includes not sharing commercially sensitive data without taking into account both the interests of the provider (or the person to whom that data relates) and the public.
Section 277A states that the provision of information under that section:
- does not breach any obligation of confidence owed by the person providing it, but
- is subject to any express restriction on disclosure imposed by any enactment (other than a restriction which allows disclosure if authorised by an enactment)
DHSC will seek to ensure that data requests comply with these principles including UK GDPR but providers should take their own legal advice as necessary.
Enforcement powers
See Adult social care provider information provisions: data enforcement for guidance on DHSC’s enforcement powers.
Annex A: reporting window periods until December 2030
The reporting window periods are:
- 8 January 2025 to 14 January 2025 (inclusive - both dates included)
- 8 February 2025 to 14 February 2025 (inclusive - both dates included)
- 8 March 2025 to 14 March 2025 (inclusive - both dates included)
- 8 April 2025 to 14 April 2025 (inclusive - both dates included)
- 8 May 2025 to 14 May 2025 (inclusive - both dates included)
- 8 June 2025 to 16 June 2025 (inclusive - both dates included)
- 8 July 2025 to 14 July 2025 (inclusive - both dates included)
- 8 August 2025 to 14 August 2025 (inclusive - both dates included)
- 8 September 2025 to 15 September 2025 (inclusive - both dates included)
- 8 October 2025 to 14 October 2025 (inclusive - both dates included)
- 8 November 2025 to 14 November 2025 (inclusive - both dates included)
- 8 December 2025 to 15 December 2025 (inclusive - both dates included)
- 8 January 2026 to 14 January 2026 (inclusive - both dates included)
- 8 February 2026 to 16 February 2026 (inclusive - both dates included)
- 8 March 2026 to 16 March 2026 (inclusive - both dates included)
- 8 April 2026 to 14 April 2026 (inclusive - both dates included)
- 8 May 2026 to 14 May 2026 (inclusive - both dates included)
- 8 June 2026 to 15 June 2026 (inclusive - both dates included)
- 8 July 2026 to 14 July 2026 (inclusive - both dates included)
- 8 August 2026 to 14 August 2026 (inclusive - both dates included)
- 8 September 2026 to 14 September 2026 (inclusive - both dates included)
- 8 October 2026 to 14 October 2026 (inclusive - both dates included)
- 8 November 2026 to 16 November 2026 (inclusive - both dates included)
- 8 December 2026 to 14 December 2026 (inclusive - both dates included)
- 8 January 2027 to 14 January 2027 (inclusive - both dates included)
- 8 February 2027 to 15 February 2027 (inclusive - both dates included)
- 8 March 2027 to 15 March 2027 (inclusive - both dates included)
- 8 April 2027 to 14 April 2027 (inclusive - both dates included)
- 8 May 2027 to 14 May 2027 (inclusive - both dates included)
- 8 June 2027 to 14 June 2027 (inclusive - both dates included)
- 8 July 2027 to 14 July 2027 (inclusive - both dates included)
- 8 August 2027 to 16 August 2027 (inclusive - both dates included)
- 8 September 2027 to 14 September 2027 (inclusive - both dates included)
- 8 October 2027 to 14 October 2027 (inclusive - both dates included)
- 8 November 2027 to 15 November 2027 (inclusive - both dates included)
- 8 December 2027 to 14 December 2027 (inclusive - both dates included)
- 8 January 2028 to 14 January 2028 (inclusive - both dates included)
- 8 February 2028 to 14 February 2028 (inclusive - both dates included)
- 8 March 2028 to 14 March 2028 (inclusive - both dates included)
- 8 April 2028 to 18 April 2028 (inclusive - both dates included)
- 8 May 2028 to 15 May 2028 (inclusive - both dates included)
- 8 June 2028 to 14 June 2028 (inclusive - both dates included)
- 8 July 2028 to 14 July 2028 (inclusive - both dates included)
- 8 August 2028 to 14 August 2028 (inclusive - both dates included)
- 8 September 2028 to 14 September 2028 (inclusive - both dates included)
- 8 October 2028 to 16 October 2028 (inclusive - both dates included)
- 8 November 2028 to 14 November 2028 (inclusive - both dates included)
- 8 December 2028 to 14 December 2028 (inclusive - both dates included)
- 8 January 2029 to 15 January 2029 (inclusive - both dates included)
- 8 February 2029 to 14 February 2029 (inclusive - both dates included)
- 8 March 2029 to 14 March 2029 (inclusive - both dates included)
- 8 April 2029 to 16 April 2029 (inclusive - both dates included)
- 8 May 2029 to 14 May 2029 (inclusive - both dates included)
- 8 June 2029 to 14 June 2029 (inclusive - both dates included)
- 8 July 2029 to 16 July 2029 (inclusive - both dates included)
- 8 August 2029 to 14 August 2029 (inclusive - both dates included)
- 8 September 2029 to 14 September 2029 (inclusive - both dates included)
- 8 October 2029 to 15 October 2029 (inclusive - both dates included)
- 8 November 2029 to 14 November 2029 (inclusive - both dates included)
- 8 December 2029 to 14 December 2029 (inclusive - both dates included)
- 8 January 2030 to 14 January 2030 (inclusive - both dates included)
- 8 February 2030 to 14 February 2030 (inclusive - both dates included)
- 8 March 2030 to 14 March 2030 (inclusive - both dates included)
- 8 April 2030 to 15 April 2030 (inclusive - both dates included)
- 8 May 2030 to 14 May 2030 (inclusive - both dates included)
- 8 June 2030 to 14 June 2030 (inclusive - both dates included)
- 8 July 2030 to 15 July 2030 (inclusive - both dates included)
- 8 August 2030 to 14 August 2030 (inclusive - both dates included)
- 8 September 2030 to 16 September 2030 (inclusive - both dates included)
- 8 October 2030 to 14 October 2030 (inclusive - both dates included)
- 8 November 2030 to 14 November 2030 (inclusive - both dates included)
- 8 December 2030 to 16 December 2030 (inclusive - both dates included)
Annex B: operational support, non-mandatory data collection
This annex contains guidance for providers on operational support, including non-mandatory data collection.
Operational support data
Operational support data items in CT are often key for local operational support and providers will be asked to update these items daily or weekly. They fall into 2 categories:
- Those that are also part of the mandatory data collection. These must be updated monthly to comply with the adult social care provider information provisions. If they are not updated, providers may be subject to enforcement. For operational support, providers are asked to update these more frequently, though this a non-mandatory request.
- Those that are not part of the mandatory data collection but for operational support, providers are asked to provide these daily or weekly, though this a non-mandatory request.
Questions that are used for operational support purposes for care home provider locations are:
- vaccination updates that are part of an ongoing campaign, for example winter flu
- daily bed vacancy updates
- if the organisation holds a sponsorship licence for international workers’ visas
- the number of Health and Care Worker and/or Skilled Worker visa holders employed under their sponsor licence
- digital social care record (DSCR) software in use, if any
- knowing who is your primary care network lead
- up-to-date infection prevention and control training
- care home rounds
Questions that are used for operational support purposes for home care provider settings are:
- vaccination updates that are part of an ongoing campaign, for example winter flu
- if the organisation holds a sponsorship licence for international workers’ visas
- the number of Health and Care Worker and/or Skilled Worker visa holders employed under their sponsor licence
- if any of their Health and Care Worker and/or Skilled Worker visa holder employees work across multiple services
- details of the multiple services the Health and Care Worker and/or Skilled Worker visa holders work across
- DSCR software in use, if any
- if they can provide any additional care hours
- the number of additional care hours they think they can provide per week
Such data requests are separate to the mandated data collection but are essential to continue to support you as providers, along with health and social care partners, such as discharge teams, to keep people and staff as safe and healthy as possible.